Table of contents
What case studies from the AWS AI Health Leaders Forum reveal about agentic workflows, trusted data architecture, and production AI in pharma and healthcare.
I recently attended the AWS AI Health Leaders Forum in Zurich. The room brought together hospital CDAOs, insurers, pharma teams, health-tech founders, and technology leaders working on some of the most difficult questions in healthcare AI.
I went there as a Life Sciences & Healthcare Advisor at deepsense.ai. I spent the last 17 years of experience across pharma, healthcare, and technology, having worked across pharma strategy, technology deployment, commercial analytics, patient pathways, and healthcare policy — including leadership roles at IQVIA, Deloitte, Delta Pharma Adria, and SoftForYou — and I’ve seen several waves of healthcare technology adoption. This one feels different.
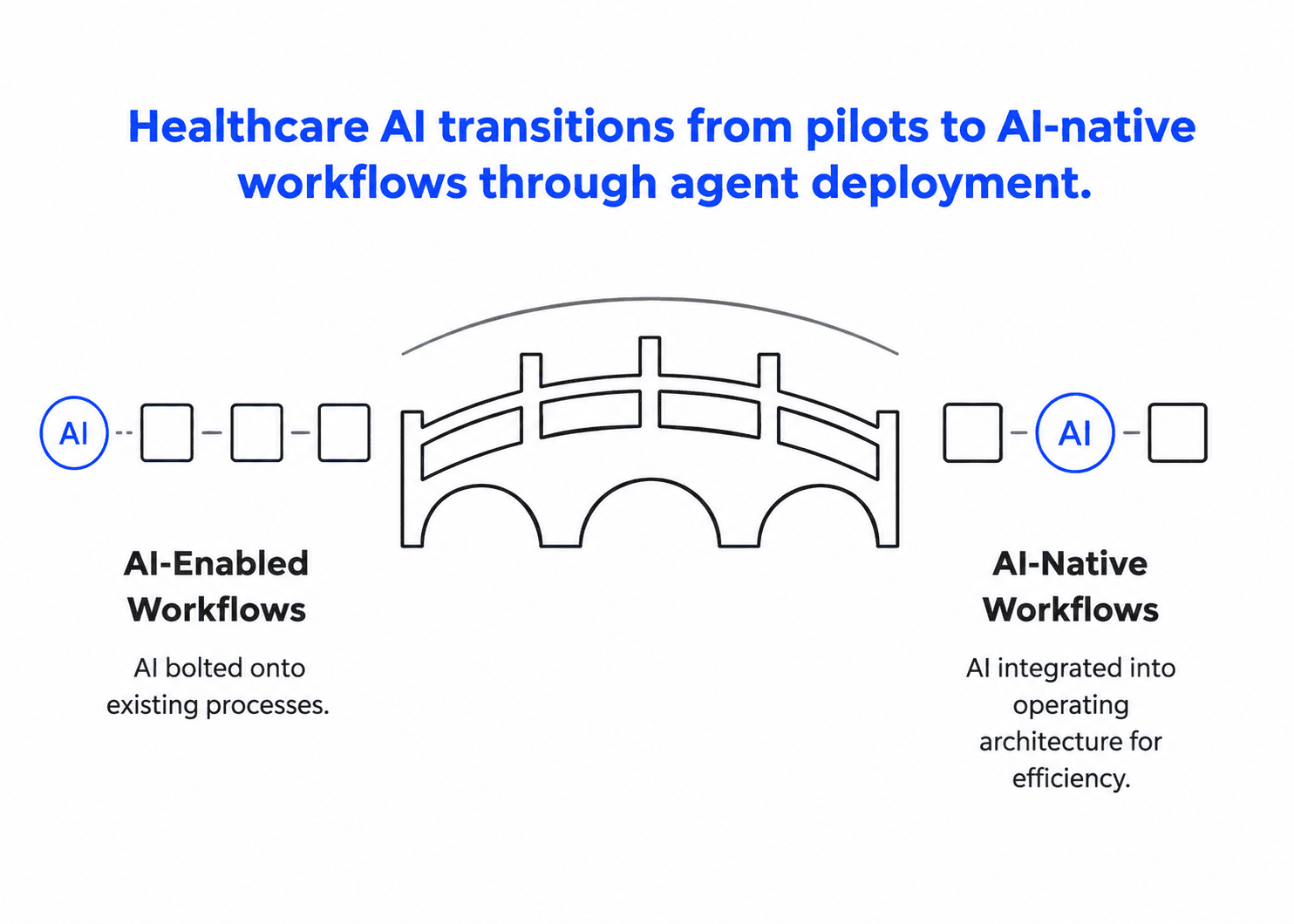
The industry has stopped debating whether AI can work in healthcare. The conversation has moved to a different question: how fast can regulated organizations move from AI-enabled workflows, where AI is bolted onto what already exists, to AI-native operating models, where AI becomes part of the architecture itself?
That shift aligns with what we see at deepsense.ai in our work with healthcare and pharma organizations, as well as with our partners such as AWS and Anthropic. The new bottleneck is the ability to connect AI safely to sensitive health and pharma data, preserve context, evaluate outputs, and make these systems trusted enough for regulated workflows.
The organizations described below are front-runners: they show what is now possible, not what is already normal. For many healthcare and pharma organizations, the pace of adoption will depend less on the models themselves and more on change management, governance, data integration, trust infrastructure, and, in some cases, regulation.
That uneven pace is worth watching in its own right. Until the field converges, adjacent organizations and systems will be operating at completely different levels. In my view, those visible gaps will become the real driver of urgency. Once patients, clinicians, and governments see the difference between what a front-runner delivers and what everyone else offers, they will simply stop accepting the lesser solutions.
For CTOs, VPs and Heads of AI in healthcare and life sciences, this has a practical consequence. AI roadmaps need to move beyond isolated copilots toward agentic workflow redesign. The highest-value targets are the workflows where knowledge, data, compliance, and expert judgment intersect. From drug discovery and clinical trials through to market access and medical affairs. It also changes what the underlying architecture has to prioritize. Evaluation, governance, data sovereignty, and ROI tracking can’t be bolted on afterward; they have to be designed in from the start.
TL;DR
- Healthcare AI is moving from pilots to production workflows. The most advanced examples in Zurich were not generic assistants but agents operating inside real healthcare, pharma, and life sciences processes.
- The key shift is from AI-enabled to AI-native. AI-enabled organizations bolt AI onto existing workflows. AI-native organizations build workflows where agents execute, humans validate, and AI becomes part of the operating architecture.
- Agents are becoming the practical unit of deployment. BARMER, IKIM / University Hospital Essen, Collective Minds, and BeeHealthy showed agentic systems applied to workflow automation, chart review, clinical trial matching, imaging review, and population health.
- The results are becoming concrete. Case studies showed 96.3% physician-accepted chart extractions, zero hallucinated values, clinical review reduced from 2 hours to 2 minutes, MVP development shortened from 9 months to 3, and +$2.1M in trial screening efficiency and accrual.
- The bottleneck is no longer only model capability. The harder problems are trusted data access, context, evaluation, governance, data sovereignty, human oversight, and workflow integration.
- For pharma and life sciences leaders, generic RAG is not enough. AI systems need domain context: biological representations, protocol and molecule history, trial criteria, safety signals, claims data, real-world evidence, clinical guidelines, and source provenance.
- The front-runners are not showing what is normal yet. They are showing what is now possible. Many organizations are still years away, and the gap will depend less on model quality than on change management, governance, data integration, policy, and trust infrastructure.
- The main takeaway: healthcare AI will scale when agents become trustworthy enough to support real clinical, pharma, and operational workflows — not when models simply become more impressive.
1. AI-enabled vs. AI-native: the distinction that framed the whole event
The clearest framing of the two days came from AWS, our partner and the forum’s host. The distinction was simple but important: most organizations are still AI-enabled, while the front-runners are moving toward AI-native operating models.
AI-enabled: AI as an add-on
In AWS’s model, an AI-enabled organization bolts AI onto an existing system.
- AI is a supporting feature, not the core architecture.
- Humans still drive most of the workflow — AWS put it at roughly 70%.
- If AI is removed, the product or process still survives.
- A better model can become a threat, because competitors can plug in the same improvement.
Many pharma and healthcare organizations are still in this camp. They have copilots, search assistants, and document automation running as pilots. These tools are useful, but they rarely change the operating model.
AI-native: AI as part of the architecture
An AI-native organization works differently.
- AI is built into the operating architecture.
- Agents execute repetitive, high-volume workflow steps.
- Humans set direction, review decision gates, validate outputs, and redirect the system.
- A better model becomes an opportunity, because it strengthens the core system.
This is where the real shift begins. The AI-native model is not about replacing experts. It is about changing the division of work: agents handle the fast, repetitive tasks such as reading, extracting, routing, generating, and escalating, while humans stay responsible for judgment, validation, and oversight.
Why this matters more in life sciences
For life sciences and healthcare, this distinction matters more than it might in other industries. The highest-value use cases are workflows where knowledge, data, compliance, and expert judgment intersect, including:
- clinical trial operations,
- medical affairs,
- regulatory intelligence,
- drug discovery,
- pharmacovigilance,
- market access,
- medical writing,
- patient engagement.
In these settings, AI has to be more than fluent. It has to be grounded, auditable, and connected to the right systems.
The infrastructure around the model becomes the real differentiator
This is also why our collaboration with Anthropic around a secure bridge between AI assistants and healthcare and pharma data systems is strategically relevant. Built on the Model Context Protocol, it addresses one of the most important adoption problems in the sector: how AI can safely and reliably use health data to create value for patients, payers, providers, and life sciences organizations.
My takeaway from Zurich was clear: the next competitive advantage in healthcare AI will not come from the model itself. It will come from the trusted, governed, evidence-grounded infrastructure around it.
2. Agents, not models, are becoming the unit of deployment
The most mature case studies in Zurich were built around agents rather than models. Two examples stayed with me because they showed what agentic AI looks like when it is treated as a production capability, not a demo.
Agent deployment as a governed capability
Germany’s largest health insurer, BARMER, with 8.7 million insured lives, presented a six-level AI Agent Maturity Model.
Its A³ program — “Agents Automate Workflows” — is explicitly designed to prove three things at once:
- agents are technically feasible,
- agents are compliant with regulation,
- agents genuinely reduce employee workload.
BARMER selected four processes, staffed more than 100 people across the business and IT, and cut MVP development time from 9 months to 3.
What I found notable was not any single number. It was that a large, conservative insurer is treating agent deployment as an industrialized, governed capability — with maturity levels and dedicated staffing — rather than as an experiment. That is what “AI-native” looks like inside a regulated institution.
And notice where BARMER places itself: Levels 2 to 3 of its own six-level model. Even a clear front-runner sees itself as partway up the curve, not at the top.
Clinical agents that read patient charts
IKIM and University Hospital Essen showed the same clinical direction. Their ACIE system reads patient charts through an orchestrated architecture, where a controlling agent coordinates sub-agents for:
- patient context,
- FHIR data,
- hospital systems,
- radiology,
- PACS,
- lab results,
- documents,
- structured extraction.
The results are the kind of clinical leaders actually respond to:
- 96.3% of 3,622 extractions were accepted by physicians who checked every value against its source,
- zero hallucinated values,
- 95.9% precision when the system answers,
- 97.1% precision when it correctly returns no answer.
In a clinical setting, a system that knows when not to answer is almost as important as one that answers well.
Agent-to-agent architecture: data is never shared, only shown
Essen’s agent-to-agent design is the part I would point pharma and hospital CTOs to.
A local records agent runs on-premises and reads patient data locally. A requesting agent on Amazon Bedrock AgentCore does the heavier reasoning. The two collaborate across an institutional boundary over guardrail-encrypted HTTPS.
The governing principle is simple and important:
Data is never shared, only shown.
This spans vendors and providers, pointing to a future of agent networks that operate across institutional and data boundaries without forcing sensitive data into a single central environment.
3. The real bottlenecks now are communication, evaluation, and context
Across the forum, the same implementation pattern recurred: the strongest barriers to adoption in healthcare and life sciences are communication, evaluation, and context.
Communication: AI as a workflow layer, not a novelty
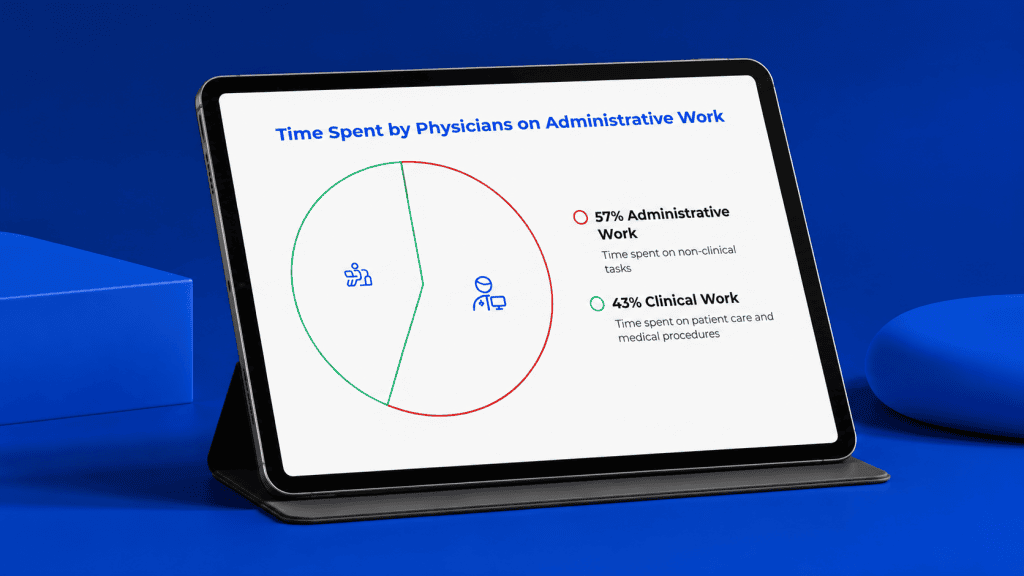
Healthcare still runs on friction in how patients, clinicians, payers, and institutions exchange information. AWS cited figures that make the point:
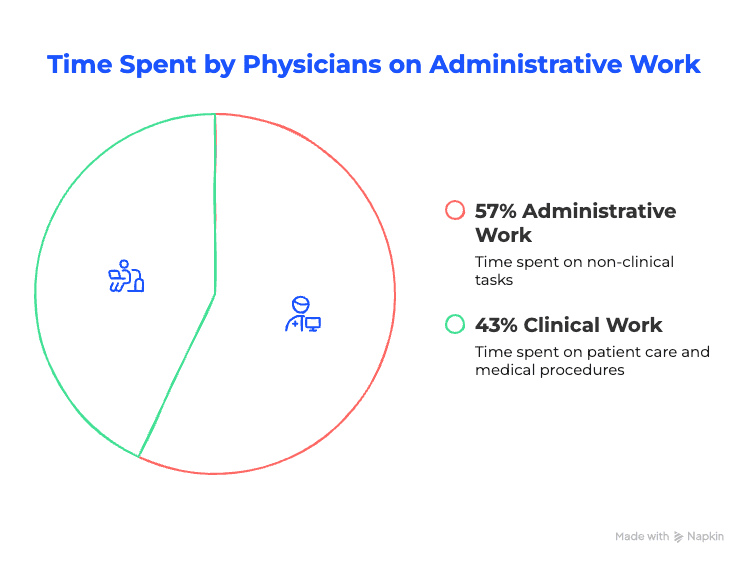
- 57% of physicians’ time is consumed by administrative work,
- 83% of patients prefer AI-enabled self-service for scheduling and routine questions,
- 71% of patients under 45 expect voice-enabled access comparable to consumer apps.
This is where voice AI stops being a novelty and becomes a workflow layer.
On the patient side, it is about:
- access,
- intake,
- follow-up,
- adherence.
On the healthcare organization side, it is about supporting:
- HCPs,
- medical liaisons,
- market access teams.
In my view, that dual use — front office and back office — is where much of the near-term value sits.
Evaluation: healthcare needs proof, not plausible answers
The fastest AI adoption of any industry is in software development. AWS put it at around 36% of all AI usage.
That is because code is verifiable: you can run it and see whether it works.
Healthcare is slower because ground truth depends on many things:
- domain expertise,
- patient context,
- clinical nuance.
The outcomes are harder to check. That is why adoption will depend on:
- evaluation frameworks,
- hallucination mitigation,
- traceability,
- human review.
In healthcare, evaluation cannot be a QA step at the end. It must be part of the product.
Context: life sciences AI needs biological representation, not only retrieval
MindWalk AI made the argument that will interest drug discovery professionals. Life sciences AI is, in their words, “starving for biological context, not data plumbing.”
Their critique of the conventional stack — ETL → vector DB → chat — is that:
- ETL joins are syntactic,
- vector search retrieves text similarity,
- program history and provenance quietly disappear.
Their alternative is a representation layer connected to biological context and reasoning layers. They describe it as:
- 660 million patterns,
- 25 billion relationships,
- built over 20 years of curation.
Their strongest proof point was the prediction of cross-reactive antibodies against all four dengue serotypes, later confirmed in wet-lab work across two independent campaigns.
The lesson for pharma leaders is direct: generic RAG is not enough. The durable advantage is the representation and context layer that lets AI reason over biology, evidence, and history — not any single model.
4. The ROI numbers are getting specific
What made the forum useful, rather than aspirational, was the specificity of the ROI claims.
Population health: €164M annual burden, €3.4M in prevented costs
BeeHealthy’s Päijät-Sote case in Finland framed population health in plain economics.
Elevated blood pressure, LDL, blood sugar, and BMI were associated with roughly €164 million a year in healthcare costs in the region.
By reaching 20% of people with risk factors and improving their treatment, the case projected:
- a 5% reduction in disease burden,
- about €3.4 million a year in prevented costs,
- 1,100 quality-adjusted life years saved annually.
Scaled to a country the size of France, that extrapolates to around €3 billion a year.
Clinical trials and imaging: +$2.1M and review time cut from hours to minutes
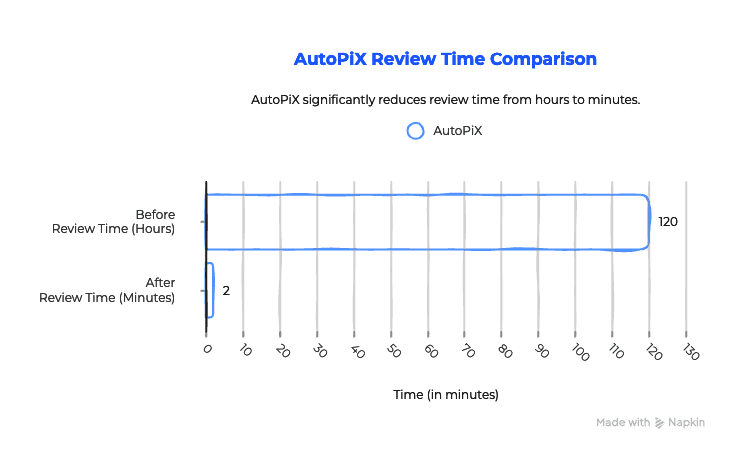
Collective Minds showed a different ROI pattern, focused on clinical trials and imaging collaboration.
Its Clinical Trial Matching Agent delivered a reported +$2.1 million in trial screening efficiency and accrual from just three use cases.
In its AutoPiX work, agentic support cut review time from two hours to two minutes, with analytics moving to near-instant.
AI delivery: MVP cycles compressed from nine months to three
BARMER’s return was organizational.
Its sprint-based development cycle compressed MVP development from nine months to three.
The practical filter: start where the baseline is measurable
Across these examples, the pattern is consistent — and useful for anyone prioritizing healthcare and life sciences AI use cases.
The best opportunities are the ones with a measurable baseline of drag:
- time lost to manual review,
- patients missed,
- trials delayed,
- evidence left fragmented.
If you cannot name the baseline you are improving, it is probably not the place to start.
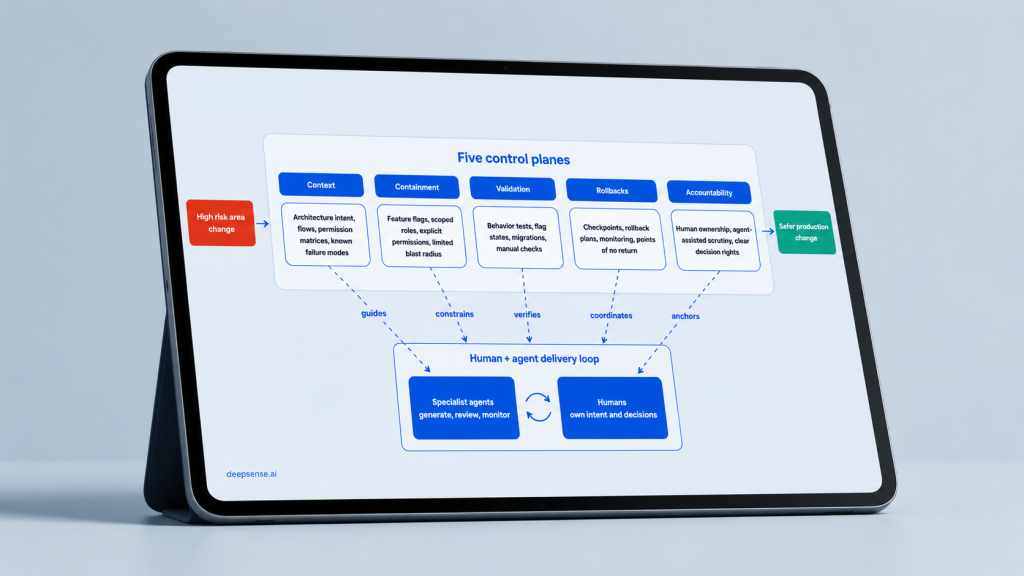
5. Trust infrastructure: evidence, provenance, and governance under every agent
If I had to name the single most important idea from Zurich, it would be this: the real advantage of healthcare AI lies in trust infrastructure.
Hospitals do not adopt black-box agents
One clinical-knowledge presentation put it bluntly: hospitals do not adopt black-box agents. They adopt agents whose reasoning traces back to trusted, citable evidence.
The stack they proposed is simple:
- trusted, referenceable medical knowledge at the base,
- patient context in the middle,
- agent capability on top.
This aligns with what IKIM demonstrated and what MindWalk argued on the pharma side. It should also shape the design of production-grade healthcare and pharma AI systems.
A clinical or pharma agent needs:
- evidence grounding,
- source citation,
- sensible no-answer behavior,
- human validation,
- audit trails,
- respect for data boundaries across hospitals, CROs, sponsors, payers, and vendors.
Data sovereignty becomes a feature, not a constraint
That last point is where data sovereignty turns from a constraint into a feature.
AWS’s European Sovereign Cloud, with its first region in Brandenburg, Germany, is described as being operated exclusively by EU residents located in the EU and backed by a €7.8 billion investment.
For regulated European health and life sciences workloads, this enables a more realistic adoption path: sensitive data can remain under appropriate jurisdictional and operational control while agents still collaborate across systems.
For a European company like deepsense.ai, that is an asset to build on, not a limitation to work around.
6. What this means for healthcare and life sciences leaders
Pulling it together, here is what I would tell a CTO, VP of AI, Head of AI, or transformation lead planning the next 12–18 months.
Move beyond isolated copilots
Copilots are fine, but the larger prize is agentic workflow redesign.
The highest-value opportunities sit in areas such as:
- Patient Access and Engagement
- Clinical Workflows
- Healthcare Operations
- Drug Discovery
- Clinical Trials
- Market Access and Medical Affairs.
Design for evaluation from the start
In regulated workflows, evaluation cannot be a final QA exercise. It belongs in the architecture.
That means building in:
- test sets,
- expert review loops,
- no-answer evaluation,
- hallucination and drift monitoring,
- source-grounding checks,
- operational KPIs.
Treat governance and data sovereignty as accelerators
Governance and data sovereignty should not be treated only as brakes.
If the architecture allows agents to collaborate while data remains protected, more use cases become viable — not fewer.
Tie ROI to a measurable baseline
The best opportunities are the ones where the pain is already quantified, such as:
- review cycles,
- call volumes,
- trial delays,
- manual extraction,
- low adherence,
- slow evidence synthesis.
If the baseline is measurable, the AI opportunity is easier to prioritize, validate, and scale.
7. Turning healthcare AI agents into reliable production systems
This is the part deepsense.ai has been building toward.
Our work is not about layering AI onto existing processes to run one more experiment. It is about turning AI into reliable systems that hold up inside real business, technical, and regulatory constraints.
Agents need to be part of production architecture
In healthcare, pharma, and life sciences, agents cannot be treated as standalone demos. They need to be designed as part of a broader production architecture, with:
- the right data access,
- clear evaluation criteria,
- source grounding,
- secure integrations,
- human oversight,
- measurable business impact.
Our recent work maps to the gaps discussed in Zurich
Recent deepsense.ai work connects directly to the challenges discussed at the forum.
We have developed:
- a secure, MCP-based bridge for Anthropic that helps AI assistants connect to healthcare and pharma data systems,
- a patient voicebot for appointment scheduling,
- key information extraction and insight analysis for a pharma company,
- evaluation frameworks for AI models.
The common thread is not experimentation. It is making AI controlled, measurable, and reliable enough for production.
The real scaling question is organizational, not only technical
The conclusion I would stand behind is the following: healthcare AI will scale when agents become trustworthy enough to run real clinical, pharma, and operational workflows.
But it will scale on each organization’s own timeline. The gating factors will often be less about technology and more about:
- change management,
- data integration,
- policy,
- trust infrastructure (evidence, provenance, and governance).
For a while, adjacent organizations will operate at very different levels. In my view, those visible gaps will become the real engine of urgency: as patients, clinicians, and regulators see the difference, the pressure to catch up or drop out will do more to move the laggards than any new model.
The front-runners in Zurich show that the destination is real. Reaching it is an organizational and sometimes regulatory project as much as a technical one — and the organizations that treat it that way will be the ones that move past pilots first.
Table of contents